Ascom, a Swiss enterprise communications company, had developed the MYCO 2: an enterprise-grade smartphone built specifically for hospital nurses. The hardware was solid. The problem was the environment it had to work in.
I joined as UX designer alongside a colleague, responsible for on-site research, concept design, user flows, wireframes, and guerrilla testing. We had a tight timeline and no room for assumptions.
- On-site user research and nurse shadowing
- Concept definition and design direction
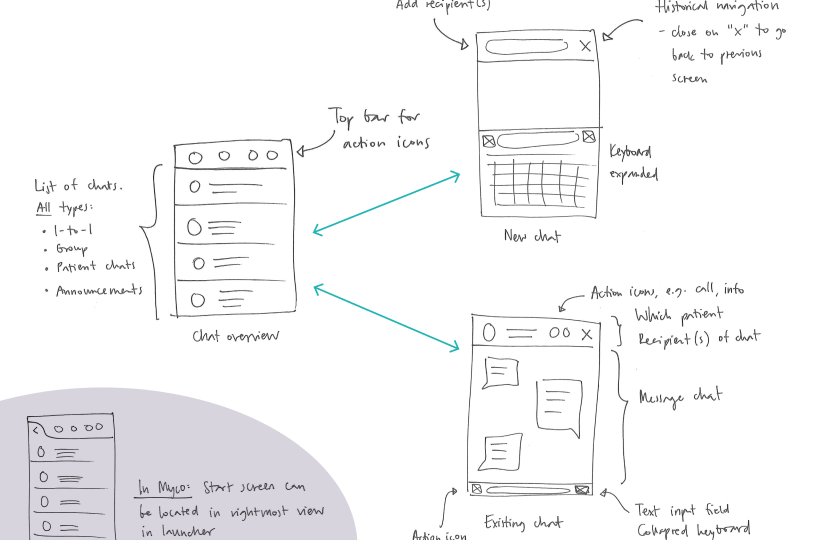
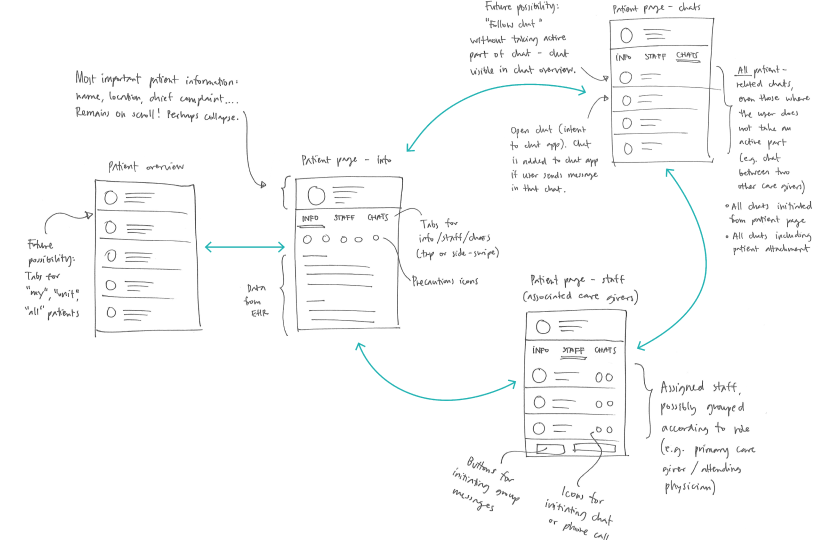
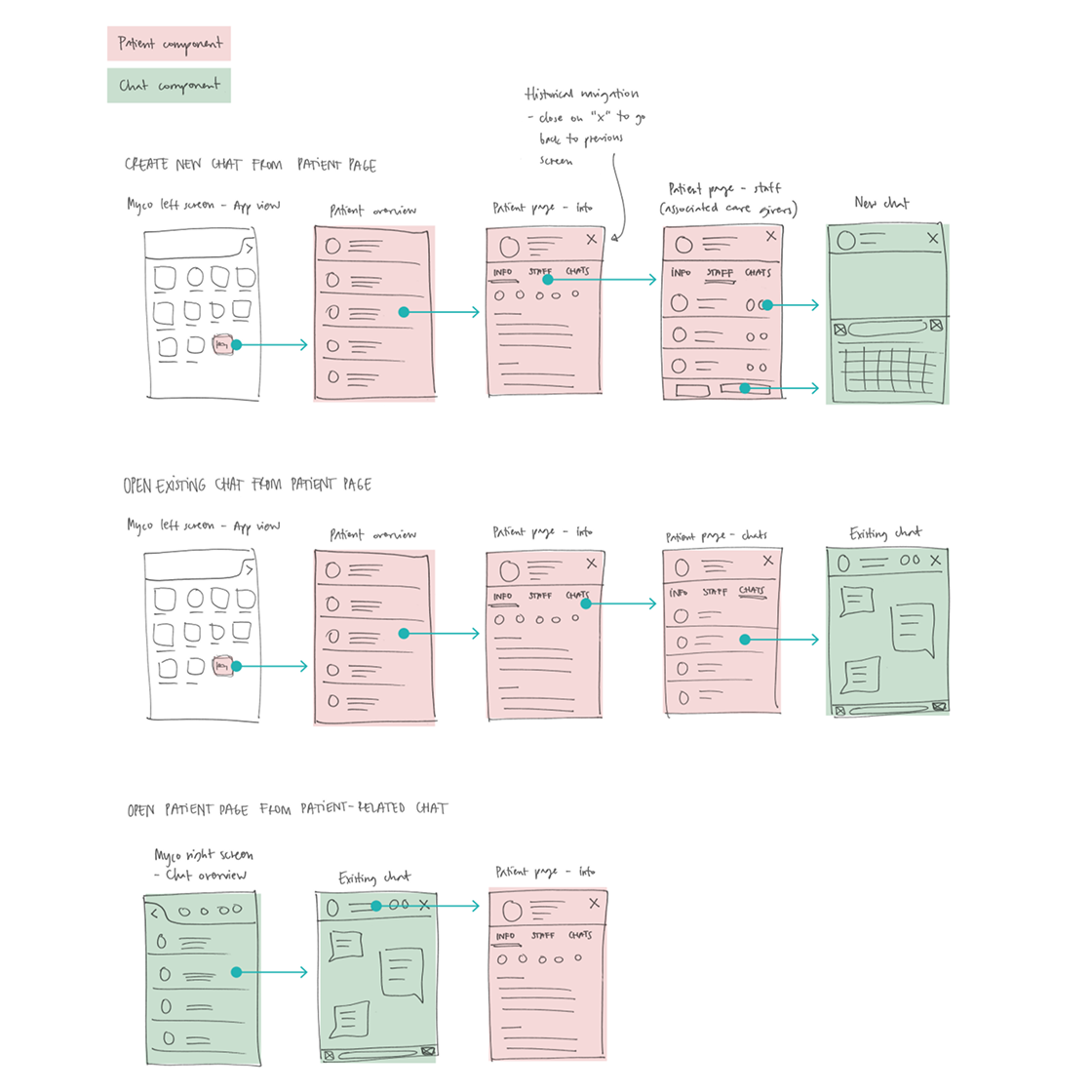
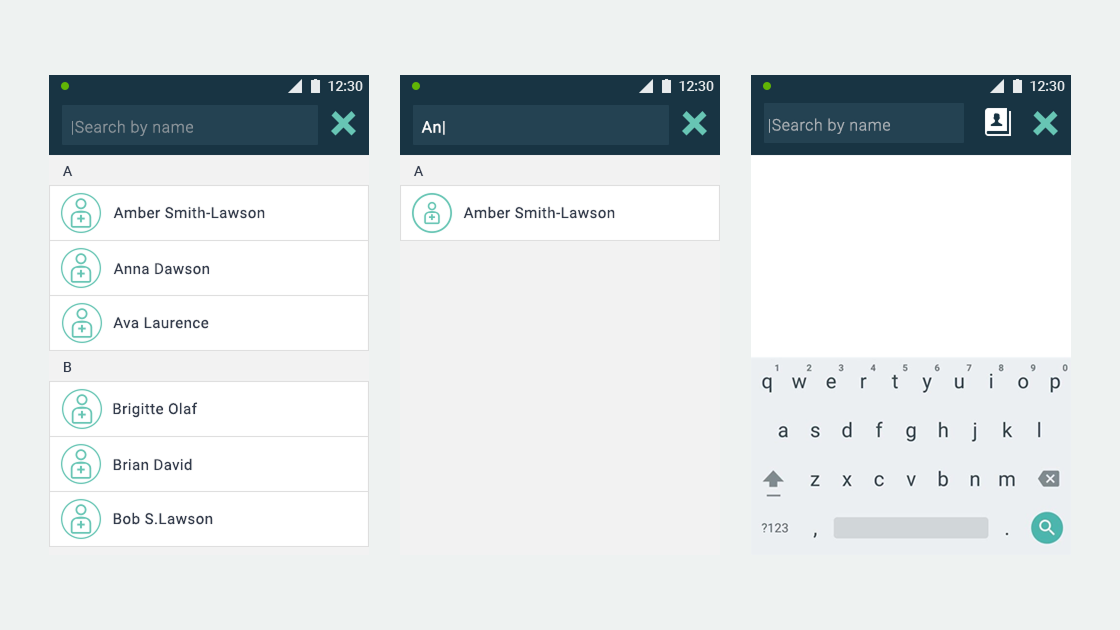
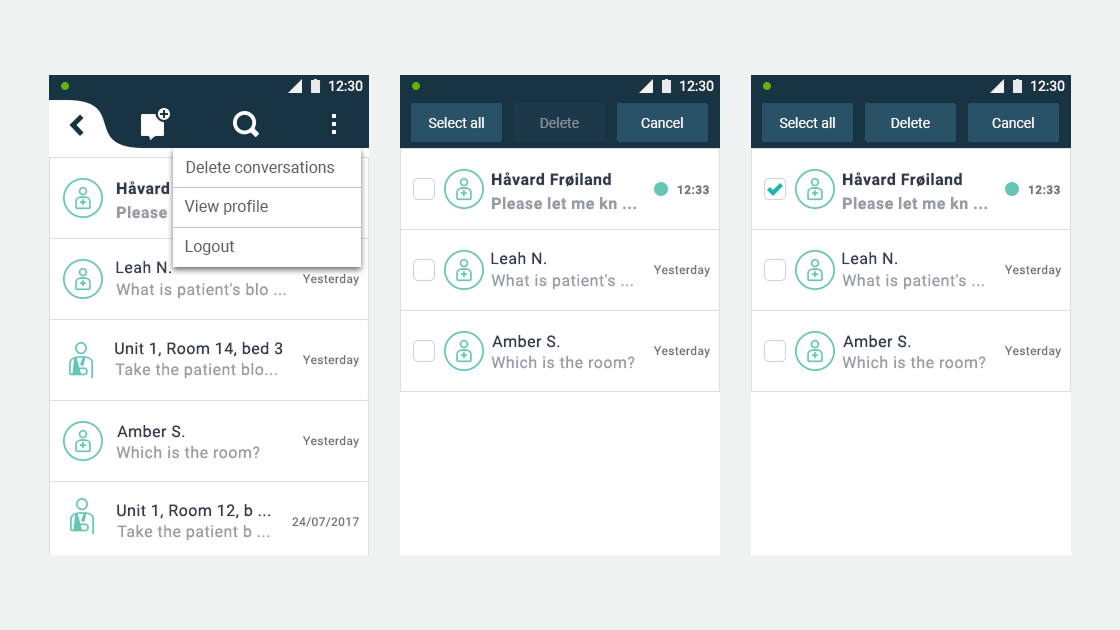
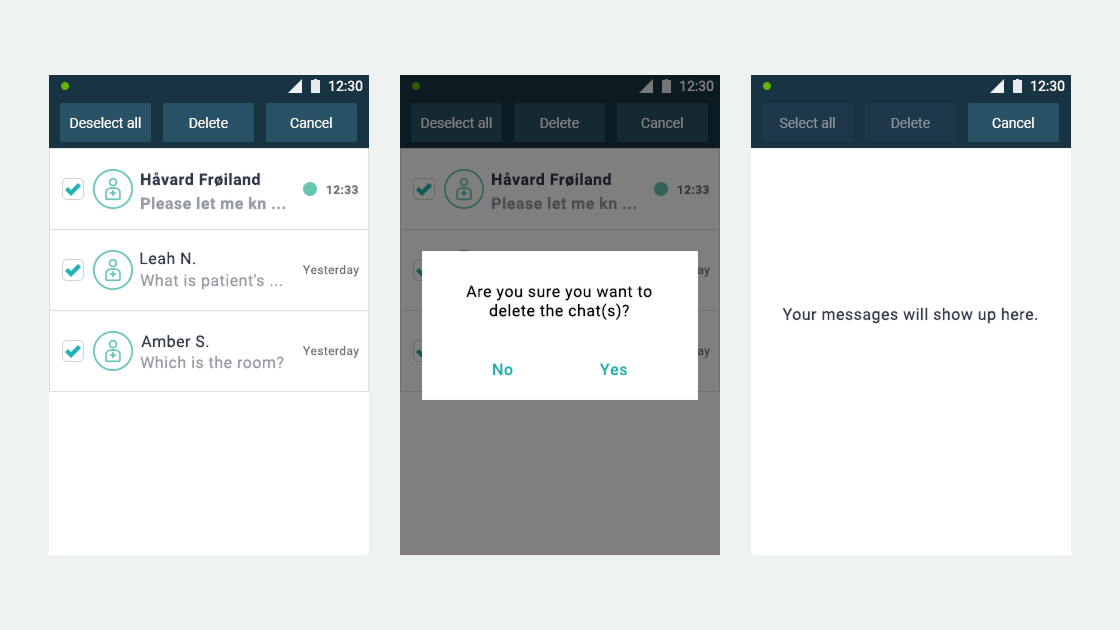
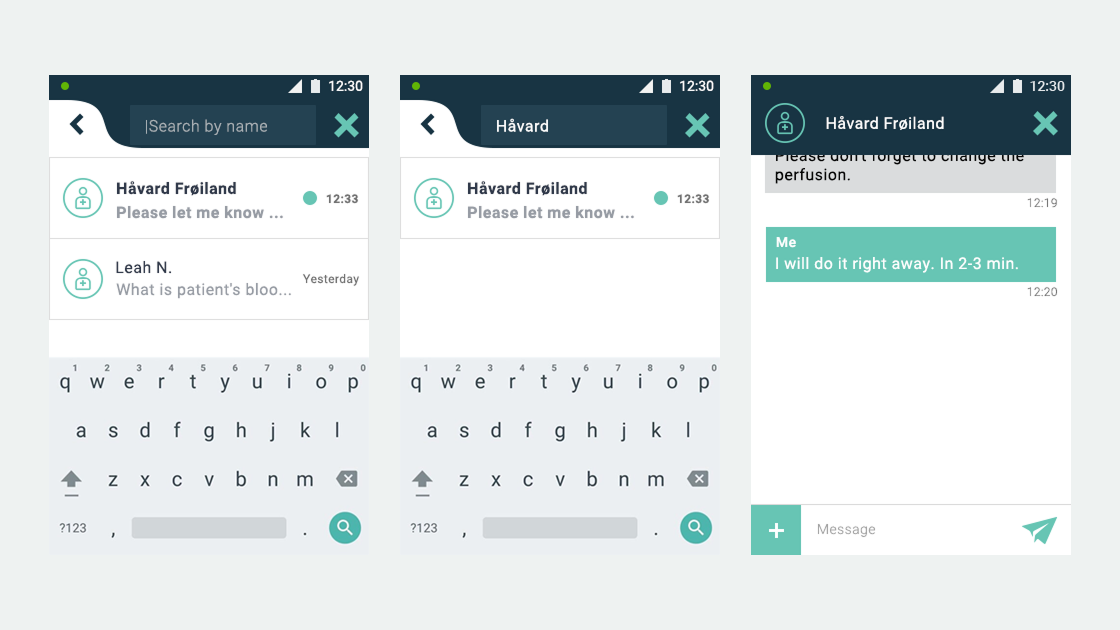
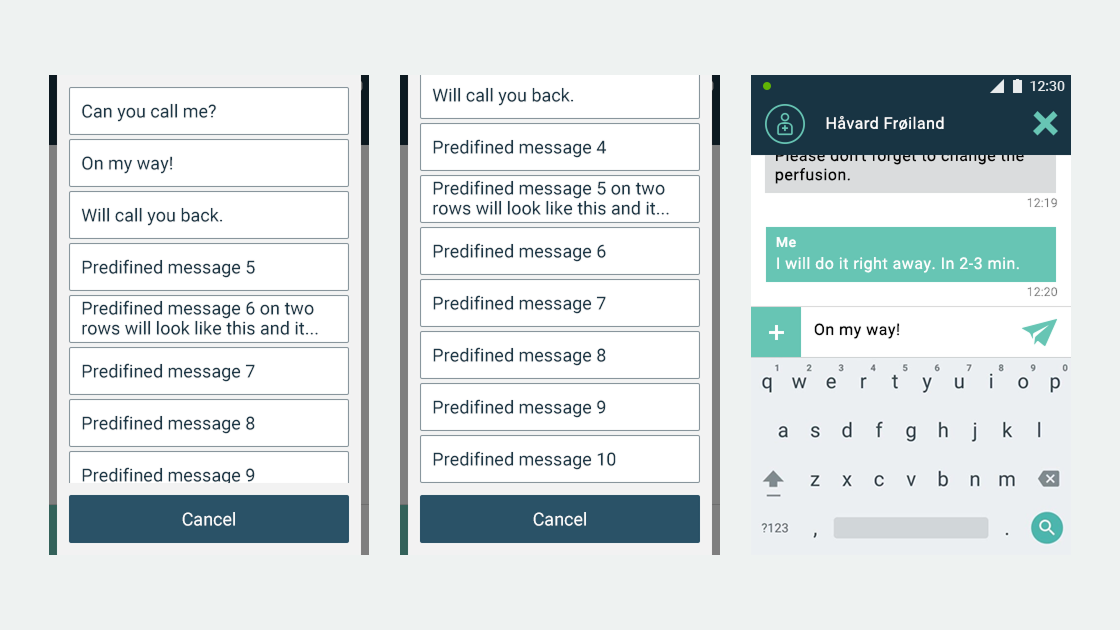
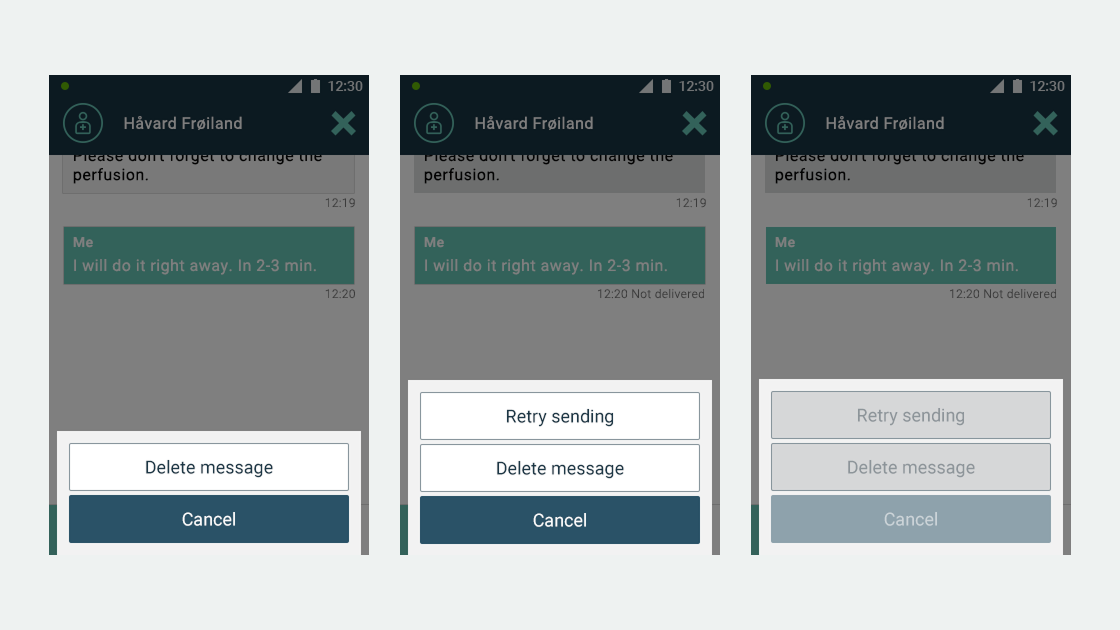
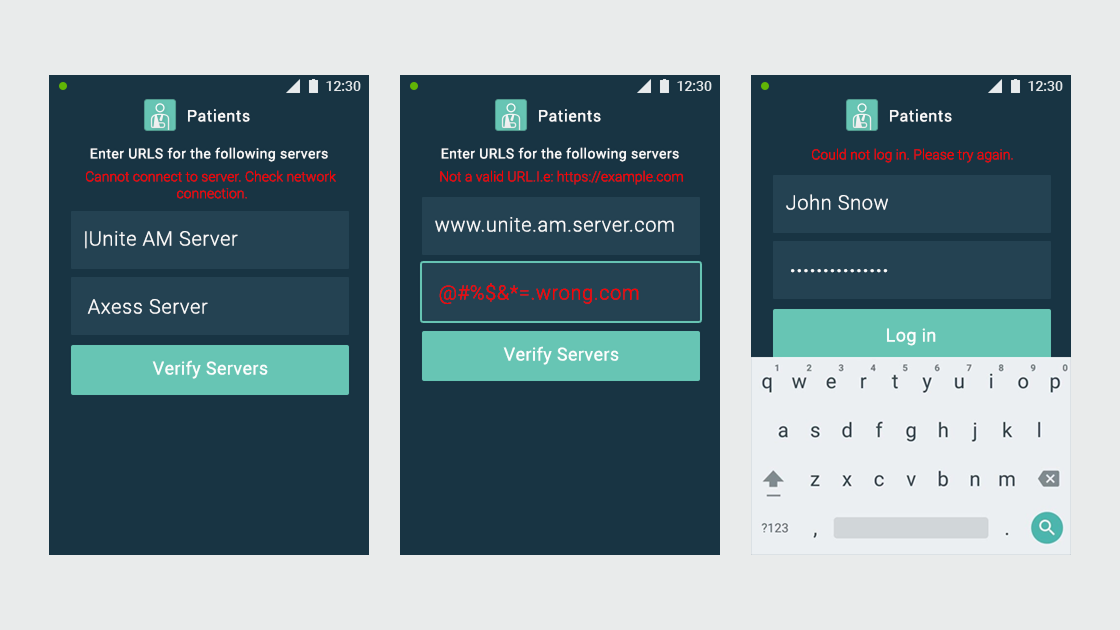
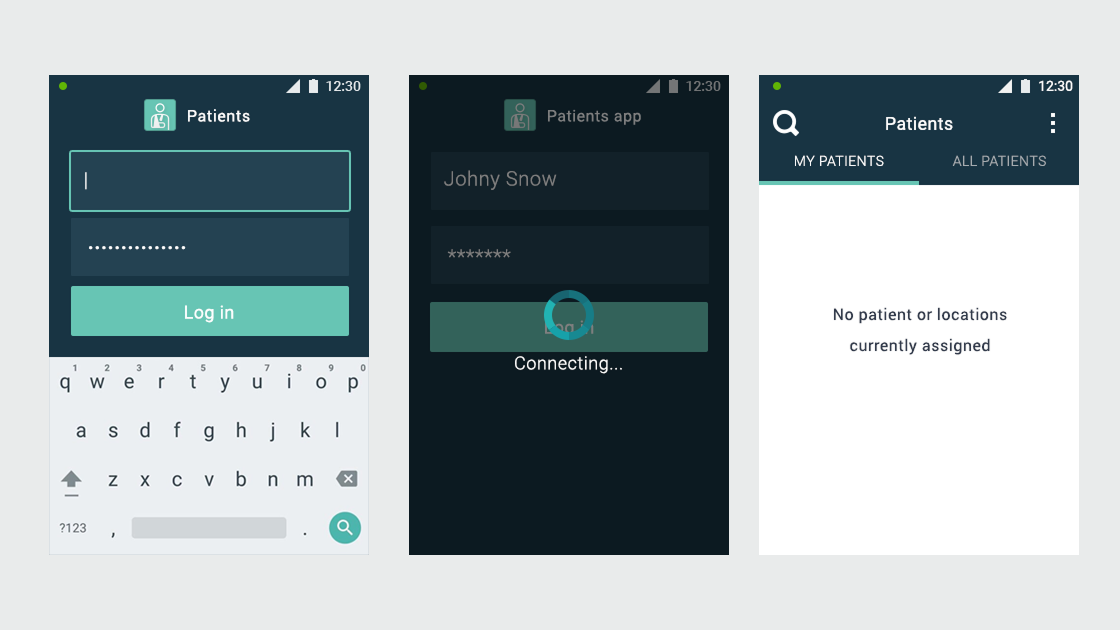
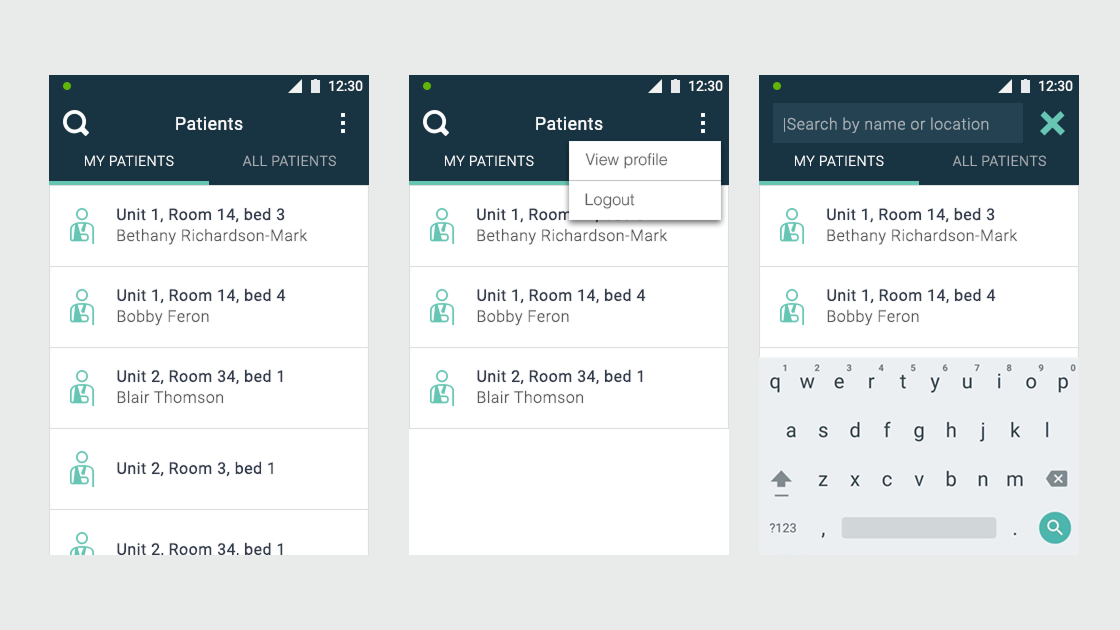
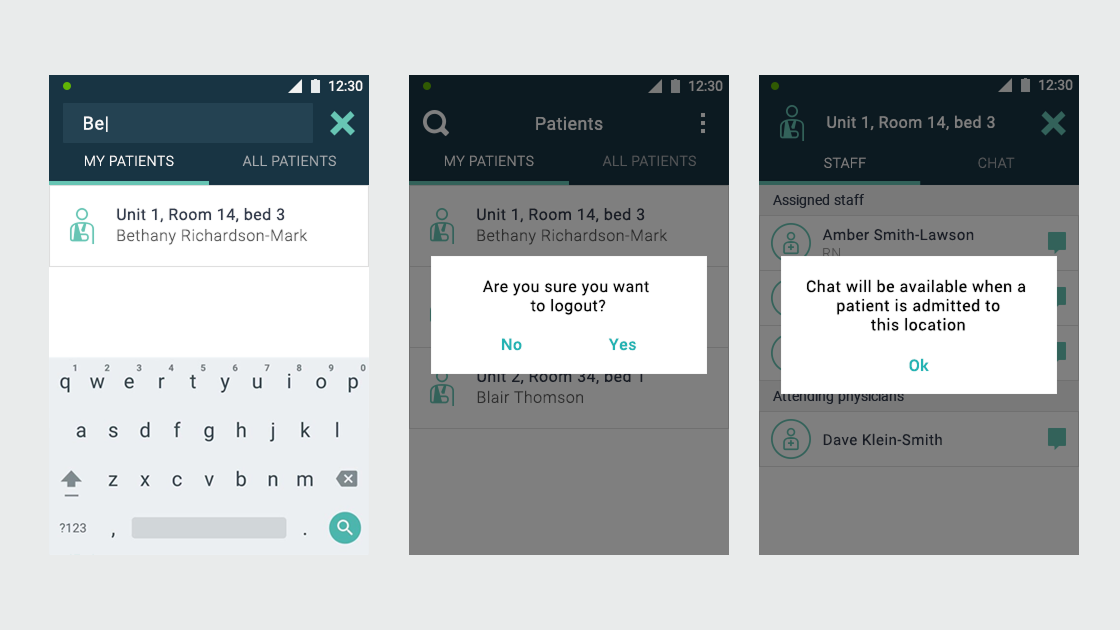
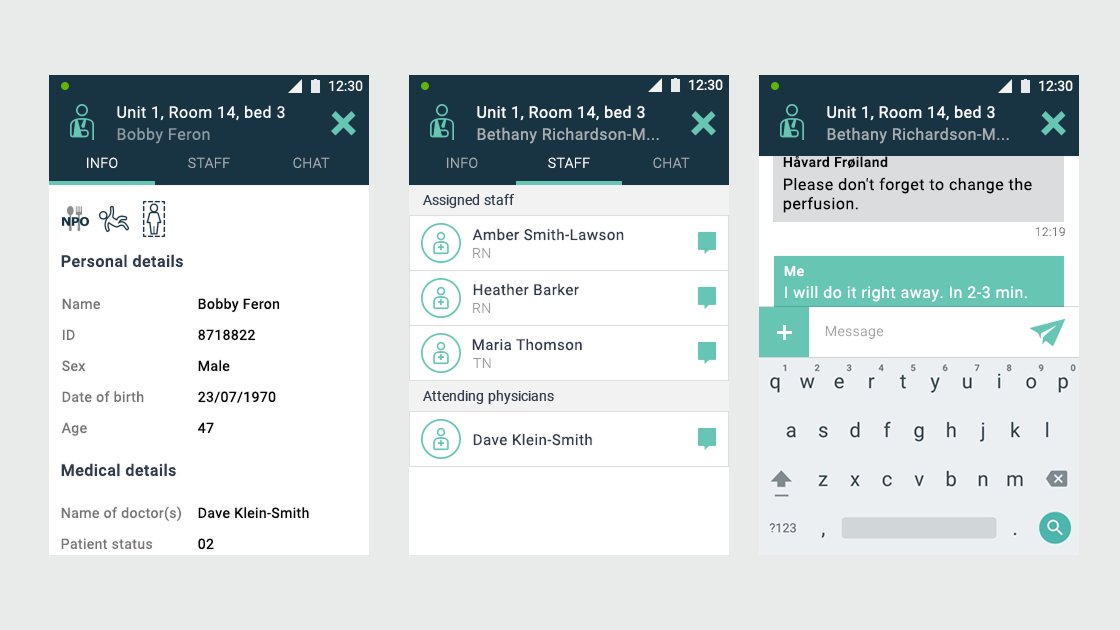
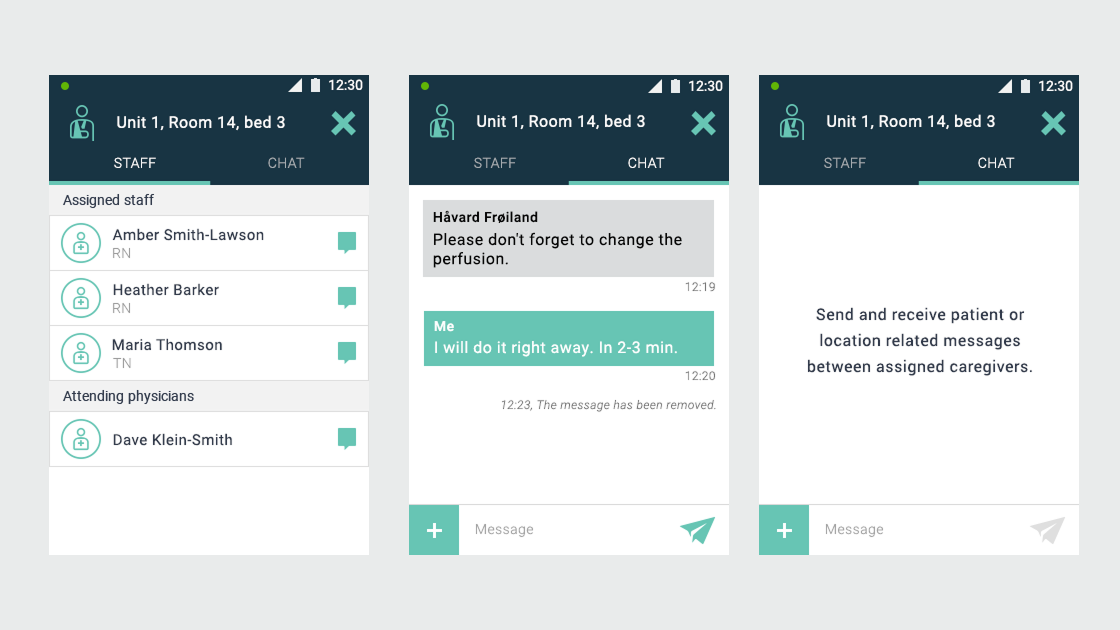
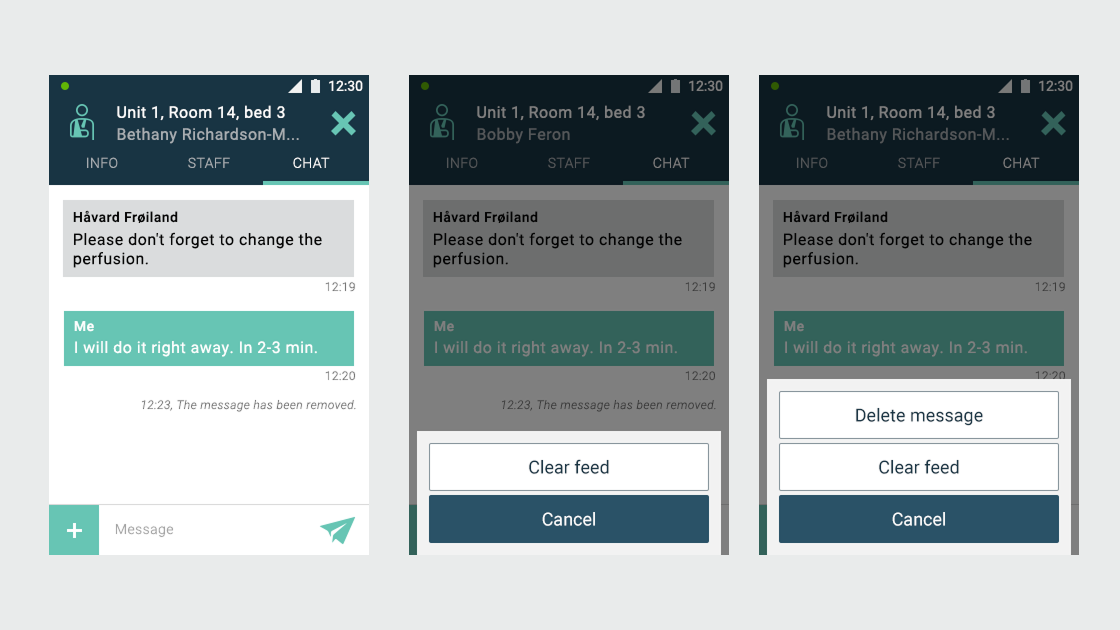
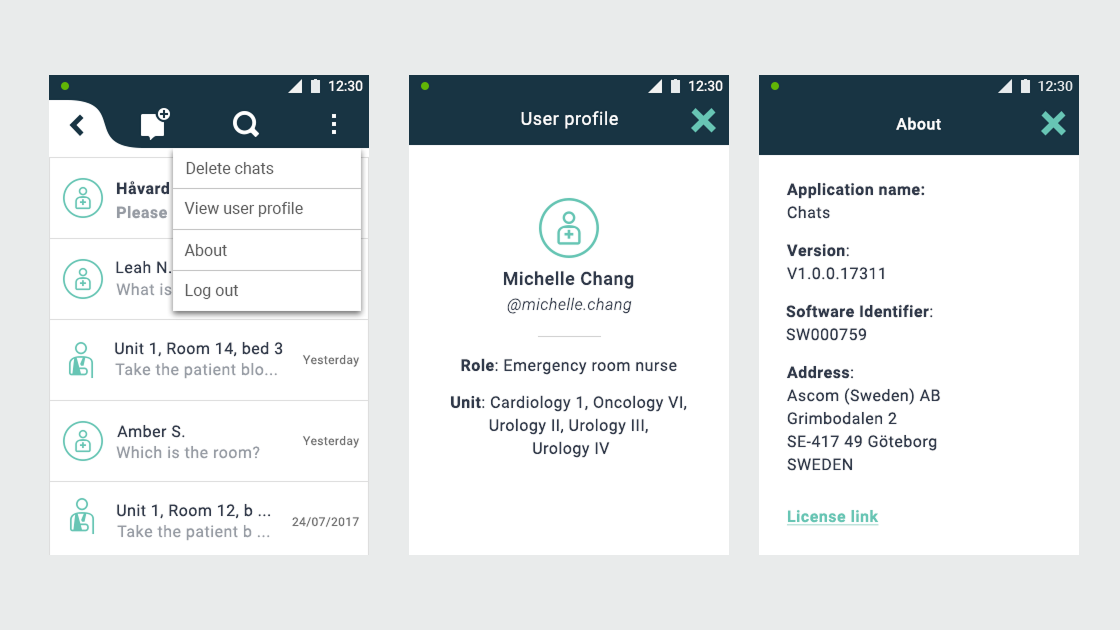
- User flows and wireframes for both applications
- Guerrilla usability testing with hospital staff